
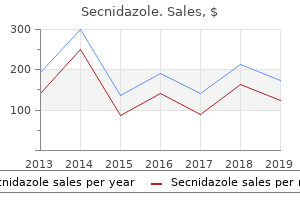
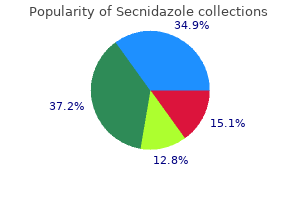
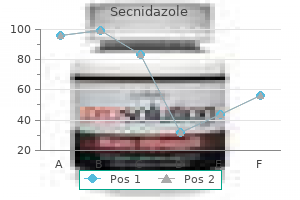
Secnidazole
"Discount 500 mg secnidazole, medications that cause hyponatremia".
By: O. Ugolf, M.S., Ph.D.
Clinical Director, State University of New York Upstate Medical University
It is desirable to have arterial and central venous access during cooling 7 medications that can cause incontinence buy secnidazole toronto, if possible symptoms bacterial vaginosis purchase secnidazole 500 mg on line. Low-dose morphine should be used to prevent agitation or shivering that occurs during therapeutic hypothermia treatment advocacy center purchase secnidazole now. Mark "severe" encephalopathy if seizures are present or if there are more signs and symptoms in the severe than the moderate column medicine pouch purchase secnidazole 1 gr on line. If the signs and symptoms are equally distributed between severe and moderate columns, the severity is based on the level of consciousness (Table 9-1). Passive cooling should be initiated at the referral hospital after the infant has been determined to be a candidate for therapeutic hypothermia, by having all heat sources removed from the infant. It is critical to tell the referring care providers to monitor temperature every 15 minutes, and if the temperature goes <33. Since energy is required to power the pump, a deficiency in cerebral energy substrates (glucose and oxygen) can lead to seizure activity. Increased availability of glutamate (an excitatory neurotransmitter) with hypoxemia, ischemia, and/or hypoglycemia can also lead to seizures. Neonates are especially prone to seizures because the mechanisms that lead to the inhibition of seizure activity are not yet fully developed. Neonatal seizures appear clinically different than seizures in children and adults due to this immaturity. Further, seizures do not progress as they do in older individuals because dendritic/axonal branching and synaptic connections are not fully developed. Since myelination is also not yet complete in cortical efferent systems, seizures may occur without motor manifestations. Further, recurrent neonatal seizures can render the brain more susceptible to the development of epilepsy later in life. In infants with encephalopathy due to a metabolic disorder, outcome will be related to the specific disorder. Similarly, outcome of encephalopathy related to an infectious etiology will depend upon the specific infection. Outcomes also can be related to maximum Sarnat stage reached which is an indication of the severity of the neonatal encephalopathy. Long-term developmental and neurologic follow-up is indicated in all cases of neonatal encephalopathy. Outcome studies from the major cooling trials have indicated that whole body hypothermia is safe, is associated with improved survival and reduced severe neurodevelopmental disability at 18 months, and the benefits noted at 18 months persist to early school age. If admitted to the Woodlands campus, developmental and neurologic follow-up should occur in the Woodlands. Subtle seizures are simply motor or autonomic changes that are not better described as clonic, tonic, or myoclonic seizures. Examples of subtle seizures include sustained opening of the eyes with fixation, chewing, pedaling motions, and apnea. Clonic seizures can be focal or multifocal and involve rhythmic jerks, usually 13 jerks per second, with the rate declining with progression of the seizure. Tonic seizures can be focal, multifocal, or generalized, and involve sustained posturing of a limb or tonic extension of extremities. Myoclonic seizures are best described as sudden jerks of muscle groups and can be focal, multifocal, or generalized. Myoclonic seizures can be distinguished from clonic seizures because of the faster speed of the myoclonic jerk and predilection for flexor muscle groups. Neonatal seizures should be distinguished from jitteriness which is non-epileptic activity. Jitteriness can appear as tremor-like movements and can be secondary to anoxic brain Guidelines for Acute Care of the Neonate, Edition 26, 201819 Section of Neonatology, Department of Pediatrics, Baylor College of Medicine Section 9-Neurology Table 9-2. If there is concern for anoxic brain injury, spectroscopy should also be performed. Also, a cranial ultrasound can detect major intracranial hemorrhages and structural abnormalities, but may not detect superficial cortical hemorrhage, such as subarachnoid bleeding.
Headaches symptoms appendicitis buy 500 mg secnidazole fast delivery, pancreatitis medicine news generic secnidazole 1 gr otc, and peripheral neuropathies are other common side effects of treatment treatment concussion cheap secnidazole 1 gr free shipping. It is Table 2 Multicomponent intervention for procedural pain management Intervention 1) Preparation 2) Relaxation and distraction Procedure Provide detailed information on the events that will follow treatment croup buy genuine secnidazole on-line. Tailor the level of information depending on the developmental level of the child. Children who are taught a specific technique such as breathing exercises believe they have more control over a painful situation, which improves pain tolerance. Mostly in the form of verbal praise, stickers, badges, sweets, or small toys that reward and encourage children to attempt to comply. One week later, the mother reports that that her child shows weakness, but the oral sores have resolved and there are no new complaints. Esophageal candidiasis is the most likely diagnosis and should be suspected on the basis of a history of difficulty in feeding and the presence of extensive thrush into the oropharynx. While mild oral candidiasis may respond well to topical therapy, the efficacy of Mycostatin drops is largely dependent on the length of time that the medication remains in contact with the lesions. It is important to explain to mothers that they need to try and remove the thick plaques that form and then apply the drops directly to the lesions (giving the drops as one would give a syrup). Alternatively, one could prescribe a gel formulation like Daktarin oral gel, which will adhere to the affected areas. Severe oral candidiasis and esophageal candidiasis will not respond to topical therapy. This is often a severely painful condition, and it is often present in infants and toddlers, causing loss of appetite or difficulty in feeding. The decision needs to be made whether the child will need to receive fluco needs to nazole intravenously, thus requiring hospital admission and possible separation from her mother, or whether the child can tolerate it orally. A child who is still taking in some oral feeds will often be able to tolerate treatment orally. As mentioned above, this condition can be extremely painful, and analgesia should also be prescribed for this patient. It is often useful to advise the mothers to try to give the dose 30 minutes before a scheduled feed so that the maximum efficacy is reached at the feed time, reducing pain on swallowing. The node continues to enlarge, causing further discomfort to the baby, and eventually it becomes red, hot, and fluctuant. The child is referred to the pediatric surgery department for incision and drainage of the node, and a course of oral prednisone is started. The surgeons then duly perform an incision and drainage (I&D) in the outpatient department. The baby is sedated with valerian syrup and is also given a dose of paracetamol (acetaminophen) prior to the procedure. The node improves, somewhat, following I&D and prednisone, but two new areas of fluctuation develop later on. The lesions are aspirated in the consulting rooms under the same sedation and analgesia as before. Also not addressed, is that the abscesses are extremely painful, particularly in an area such as the axilla, which will be manipulated during dressing, transportation, and so on. This process allows the pus to be drained to the surface and prevents sinus formation as well as relieving the pain of the abscess itself. Unfortunately, inadequately aspirated abscesses often recur with resultant recurrence of pain. It is difficult to adequately aspirate large abscesses, particularly those which have been present long enough to begin develop into separate locations. In some cases this method is preferable to the outpatient procedures for children as the pain of the procedure is completely dealt with by the anesthetic. It allows the abscess to be completely drained and to ensure that all septae are broken for good drainage. On the other hand, general anesthesia requires that the child be separated from her mother, admitted to hospital, and exposed to an unfamiliar and scary operating room. And, of course, the postoperative pain still has to be managed, just as for the outpatient procedure. What are some possible things that could have been done to have prevented this state of affairs? While it is often traumatic for parents to watch blood being drawn from their child, it is more often more traumatic for the child to face the procedure alone feeling abandoned by their mother, whom they trust to protect them from pain.
Gas trapping can occur if ventilator rates greater than 20-30/min are employed in face of severe treatment vs cure order secnidazole without a prescription, uneven airway obstruction medications zolpidem purchase secnidazole online from canada. Reductions in FiO2 or ventilator support should be done in small increments with several days of observation for signs of deterioration between weaning of each parameter medicine for yeast infection cheap secnidazole 1 gr visa. Over time treatment plant cheap secnidazole 500mg mastercard, lung growth and remodeling result in increasing stability of oxygenation and improving lung mechanics. Weaning must be done carefully because several days may be required for these patients to exhibit signs of clinical deterioration after a small reduction in level of support. This may reduce airway distension during tidal ventilation and potentially reduce airway injury. Current evidence does not demonstrate any long-term benefits for this strategy when compared to rescue use. Although short-term improvement in oxygenation or patient status at 28 days of age has been reported, metaanalysis of studies using the current recommended lung recruitment strategy has not demonstrated any superiority in long-term survival, neurologic status, or lung function. Physiology Gas exchange on the oscillator appears to result from bias flow in the airway tree induced by the high-frequency pulsations as well as by enhancement of molecular diffusion. These effects are superimposed upon the usual mechanisms of pendelluft, cardiogenic mixing, and convective flow to short pathway lung units. The basic concepts of the three-compartment lung model remain operative in oscillator decision making. In multicenter studies, the average Paw for initial treatment was 11 to 19 cm H2O, however some patients may require higher levels. These disorders have uneven expiratory time constants and therefore at increased risk of gas trapping. Inadvertent increases in lung volume and intrapleural pressure associated with improving compliance could decrease venous return and circulatory function, increase cerebral vascular congestion, or result in air leak. For most clinical situations, only mean airway pressure (Paw) and oscillatory pressure amplitude (P) are varied. Bias flow, piston centering, and percent inspiratory time are set initially and rarely vary throughout the course. In the Provo Multicenter Trial (surfactant + high volume strategy), average P for initial treatment was 23 cm H2O. Sudden, unexplained bradycardic events that occur with no other demonstrable cause might signal rapid improvement in lung compliance and the need to wean pressures more aggressively. Patient and head position should be rotated every 12 hours to avoid pressure injuries to the skin and dependent atelectasis. Wean to conventional ventilation when: air leak, if present, has resolved, Paw has been weaned to the 10- to 12-cm range, P has been weaned to less than 30 cm, and blood gases are stable. The general strategy is to recruit and maintain normal lung volume using relatively high Paw during the acute phase of lung disease. There is obliteration of small pulmonary arterioles, smooth muscle proliferation, diminished angiogenesis and abnormal vasoreactivity. A 3-compartment model can be used to describe the complex disease heterogeneity and fragile heart-lung interaction in these patients. In the first compartment, there is destruction of the small airways, airspace-capillary interface, and blood vessels, effectively reducing the cross-sectional area of the pulmonary vascular bed and gas exchange surface. This leaves the third compartment, with relatively well-ventilated lung units and intact vasculature, having to accept a disproportionate amount of pulmonary blood flow. The blood vessels of this compartment, already maximally dilated, can accept this additional flow only at the expense of high right ventricular afterload, high microvascular pressures (in both pulmonary and systemic circuits), and resultant fluid filtration into the perivascular interstitium. The chronically elevated pressures also inhibit and overwhelm pulmonary and systemic lymphatic drainage mechanisms. Any further reduction in ventilation or fall in PaO2 in the underventilated compartment. Understanding this fragile heart-lung interaction is critical in patient management. This prevents the vicious cycle of pulmonary edema causing deterioration in pulmonary function, increasing hypoxemia time and progressive worsening of pulmonary hypertension. If unchecked, such a course can result in cor pulmonale, right ventricular failure, and death. Prenatal factors include placental dysfunction, fetal growth restriction, chorioamnionitis, and genetic predisposition.
The overall prenatal detection rate for gastrointestinal obstruction is 34%; it is 52% for duodenal symptoms mononucleosis purchase secnidazole online pills, 40% for small intestine treatment xerophthalmia effective secnidazole 500mg, 29% for large intestine symptoms 5 weeks pregnant order secnidazole 1gr online, 25% for esophageal symptoms whiplash order generic secnidazole on line, and 7% for anal atresia. Most trials involve internal or external obstruction of the trachea, which allows expansion of the lungs in utero. Trials have been limited by concerns regarding maternal safety, premature labor, and miscarriage. Myelomeningocele: Prenatal repair for myelomeningocele reduced the need for shunting and improved motor outcomes at 30 months but was associated with maternal and fetal risks. Twin-twin transfusion syndrome: In monochorionic twins with evidence of unequal distribution of blood flow between fetuses, fetoscopic laser surgery can be performed to disconnect some of the communicating blood vessels in utero. This procedure stops the flow of blood from the donor to the recipient and halts the progression of twin-twin transfusion. This has led to the performance of either fetal surgical resection of the massively enlarged pulmonary lobe (fetal lobectomy) for cystic or solid lesions or thoracoamniotic shunting for lesions with a dominant cyst. It was discovered that administration of betamethasone, performed preoperatively to induce fetal lung maturity, also caused regression of these lesions. Sacrococcygeal teratoma: Fetuses with evidence of hydrops have been treated with trials of radiofrequency ablation of feeding vessels or fetal resection of the teratoma. A randomized controlled trial of fetal endoscopic tracheal occlusion versus postnatal management of severe isolated congenital diaphragmatic hernia. Changing perspectives on the perinatal management of isolated congenital diaphragmatic hernia in Europe. The posterolateral portion of the diaphragm is the last to form, when the pleuroperitoneal canal closes. Although affected infants will occasionally be asymptomatic, they usually present with moderate to severe respiratory distress. There are diminished breath sounds on the side of the hernia and usually a shift of the heart and trachea to the opposite side. Prenatal lung-head ratio: threshold to predict outcome for congenital diaphragmatic hernia. Liver position and lung-to-head ratio for prediction of extracorporeal membrane oxygenation and survival in isolated left congenital diaphragmatic hernia. Left-sided diaphragmatic hernia with air-filled loops of intestine on the left side of the chest and deviation of the mediastinum to the right. Endotracheal intubation with mechanical ventilation, supplemental oxygen, and orogastric decompression are used immediately in the presence of respiratory distress. Positive pressure ventilation through a face mask is not recommended because gas will enter the gastrointestinal tract and further compress the lungs. Exogenous surfactant, high-frequency ventilation, and inhaled nitric oxide are occasionally used but have no proven benefit. Protocolized management of infants with congenital diaphragmatic hernia: effect on survival. Congenital diaphragmatic hernia and protective ventilation strategies in pediatric surgery. Permissive hypercapnia in the management of congenital diaphragmatic hernia: our institutional experience. Postnatal management and long-term outcome for survivors with congenital diaphragmatic hernia. Most of the improvement is believed to be attributable to referral to high-volume tertiary care centers for management of these babies, as well as minimization of iatrogenic pulmonary injury through the avoidance of high ventilatory settings. Long-term follow-up in high risk congential diaphragmatic hernia survivors: patching the diaphram affects outcome. Mechanical ventilation strategies in the management of congenital diaphragmatic hernia. A cannula is placed into the right atrium via the right internal jugular vein for venous return, and a second cannula is placed into the aortic arch by way of the right common carotid artery for arterial delivery. In cases of isolated respiratory failure such as in meconium aspiration, venovenous support can be used. A double-lumen cannula is placed into the right internal jugular vein, and the tip of the cannula lies in the right atrium. Relative contraindications that must be considered are the presence of an irreversible cardiopulmonary disorder, coexisting anomalies incompatible with life.
Purchase secnidazole toronto. Alan Watts ~ Why We're So Depressed....